
How This Model Restores Trust in Public Health
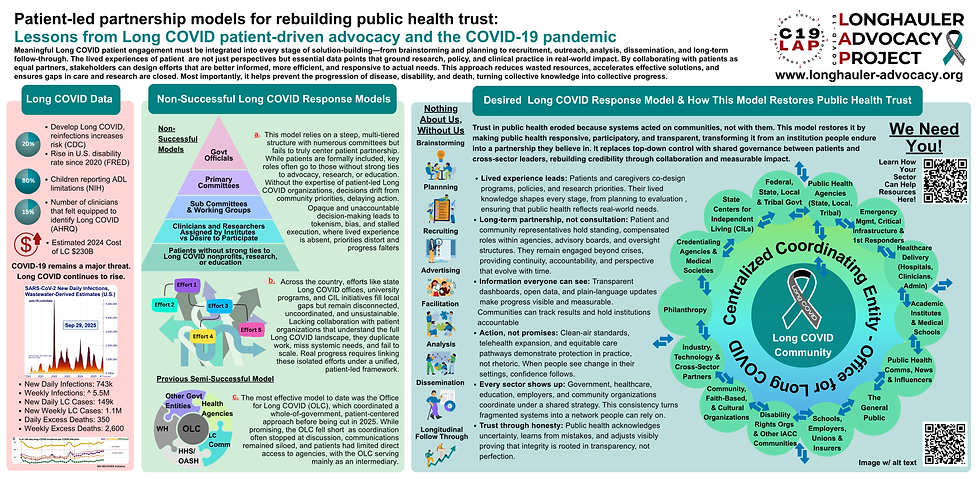
Trust in public health eroded because systems acted on communities, not with them. This model restores it by making public health responsive, participatory, and transparent, transforming it from an institution people endure into a partnership they believe in. It replaces top-down control with shared governance between patients and cross-sector leaders, rebuilding credibility through collaboration and measurable impact.

-
Lived experience leads: Patients and caregivers co-design programs, policies, and research priorities. Their lived knowledge shapes every stage, from planning to evaluation, ensuring that public health reflects real-world needs.
-
Long-term partnership, not consultation: Patient and community representatives hold standing, compensated roles within agencies, advisory boards, and oversight structures. They remain engaged beyond crises, providing continuity, accountability, and perspective that evolve with time.
-
Information everyone can see: Transparent dashboards, open data, and plain-language updates make progress visible and measurable. Communities can track results and hold institutions accountable.
-
Action, not promises: Clean-air standards, telehealth expansion, and equitable care pathways demonstrate protection in practice, not rhetoric. When people see change in their settings, confidence follows.
-
Every sector shows up: Government, healthcare, education, employers, and community organizations coordinate under a shared strategy. This consistency turns fragmented systems into a network people can rely on.
-
Trust through honesty: Public health acknowledges uncertainty, learns from mistakes, and adjusts visibly proving integrity is rooted in transparency, not perfection.

2025 Long COVID Public Health Resources
Join the National Public Health Response to Long COVID
Long COVID is a national public health crisis affecting an estimated 60 million Americans, or 20% of people who contract COVID-19. The risk increases with each reinfection, and the effects span every age group. Among children with Long COVID, over 80% report limitations in activities of daily living (ADLs), and Long COVID has now surpassed asthma as the leading chronic illness among U.S. children. This is reshaping both current and future generations.
The consequences are staggering: U.S. disability rates have risen 20% since 2020, closely mirroring Long COVID prevalence. An AHRQ study found that only 15% of clinicians felt equipped to identify Long COVID in their patients leaving millions undiagnosed, untreated, and unsupported. The annual economic cost of Long COVID is estimated in the hundreds of billions of dollars, including healthcare costs, lost income, and productivity losses, threatening the stability of our workforce and economy.
National Momentum Is Building — and Bipartisan: Recent signals from HHS Secretary Kennedy, Senators Todd Young and Roger Marshall, and Congressman Jack Bergman reflect a new wave of bipartisan support for coordinated action on Long COVID, building on the sustained leadership of champions who have supported this work from the start. This moment offers a rare opportunity for unified, cross-party collaboration on one of the most urgent and complex public-health challenges of our time.
Why Now: Each day of inaction compounds the human and economic toll. Every reinfection increases risk, and the systems built to manage acute COVID-19 are now strained by its long-term consequences. We cannot afford to wait for federal solutions—state, local, and cross-sector leadership must mobilize now.
Resources & Infographics:
-
A National Public Health Response to Long COVID: Guidance for Cross-Sector Stakeholders
-
Poster & PowerPoints showcasing scalable implementation models
-
Who Is C19LAP — our mission, national reach, and impact
-
Nothing About Us, Without Us — centering lived experience in public-health response
-
NASEM Long COVID Definition & Report (adopted by HHS in 2024)
-
C19LAP Comprehensive Guide to Long COVID — the leading reference for clinicians & policymakers
-
Downloadable Infographics for education, awareness, and prevention
Take Action:
-
Connect on TAPT: Exchange contact information & leave a google review
-
Request a Meeting with C19LAP to explore collaboration
-
Express Interest in Joining a Long COVID Public Health Network
-
Recommend C19LAP’s Involvement in Long COVID or pandemic-related initiatives
-
Connect with Our Community to learn, share strategies and resources
-
Support Our Mission to advance education, equity, and recovery
Every Sector Has a Responsibility in Long COVID
-
Patient & Caregiver Community – The foundation of the Long COVID response; identifies emerging symptoms, care gaps, and systemic failures in real time.
-
Federal, State, Local & Tribal Government – Controls policy, funding, infrastructure, and protections.
-
Public Health Agencies (CDC, NIH, HRSA, FDA; State/Local/Tribal Health Departments) – Lead surveillance, prevention, and coordination of the Long COVID response.
-
Emergency Management & First Responders – Maintain operational continuity and protect essential services.
-
Healthcare Delivery (Hospitals, Clinics, Clinicians, Administrators) – The first point of contact; determine whether patients are believed, diagnosed, and treated.
-
Academia & Medical Schools – Educate the workforce and produce the evidence base for care.
-
Credentialing Agencies & Medical Societies – Define clinical standards and competencies across specialties.
-
Schools, Employers, Unions & Insurers – Gatekeepers of inclusion, accommodations, and benefits.
-
Community, Faith-Based & Cultural Organizations – Trusted anchors connecting institutions and marginalized communities.
-
Industry, Technology & Cross-Sector Partners – Drive innovation, data infrastructure, and therapeutics.
-
Public Health Communication & Media – Shape public understanding, trust, and behavior.
-
Philanthropy & Funding Partners – Provide rapid, flexible, and sustaining resources for innovation and equity.
-
Disability Rights & Centers for Independent Living (CILs) – Enforce access, accommodations, and protections under disability law.
-
General Public – The engine of prevention, accountability, and culture.
A National Public Health Response to Long COVID: Guidance for Cross-SectorStakeholders
Long COVID is not a niche condition, it is a mass disabling event and an ongoing public health crisis. Tens of millions of Americans are affected, driving workforce losses, school disruptions, inequities, and record disability claims. Delayed care and clinician shortages compound the crisis, while public trust in institutions continues to erode.
Whether this moment becomes a turning point or a prolonged national failure depends on coordinated, cross-sector action with patients and caregivers at the center. Public health professionals hold the power to transform advocacy into infrastructure and build a sustainable, equitable response.
The goal is unified, cross-sector advocacy: one message, many voices, coordinated action. See our detailed Guide here for more info.!

Poster & PowerPoints
.png)


Who Is C19LAP
The COVID-19 Longhauler Advocacy Project (C19LAP) is a grassroots, patient-led 501(c)(3) nonprofit organization founded in June 2020 to advance the understanding of Long COVID and its associated conditions and expedite solutions and assistance to Longhaulers and their families through advocacy, education, research, resource development, cross-sector collaboration, and peer support.
C19LAP believes that education is the foundation of all meaningful progress in the Long COVID space. Our work prioritizes education and resource development, drawing on the collective lived experience of patients and caregivers, as well as deep cross-sector collaboration.
What began as a single Facebook group has grown into a nationwide network with over 60 state, territorial, and community-based chapters. Today, C19LAP is the longest-standing patient-led Long COVID nonprofit organization in the country and uniquely positioned to lead the future of Long COVID as a trusted resource across government, academia, and clinical communities, with formal leadership roles across past and present federal efforts and other key Long COVID initiatives.
In the absence and loss of Long COVID programs, our leadership role is more important than ever to bridge the gaps in action, barriers faced, and development of new and more successful initiatives driving solutions. C19LAP is consistently educating those on the front lines and helping to inform national policy and research through education and direct collaboration with scientists, public health leaders, policymakers, and most importantly, our community.
Initiatives We Have Participated In
-
National Academy of Sciences, Engineering, and Medicine- 2024 Consensus Long COVID Definition, Adopted by HHS
-
Our early research led to the Memorandum on Long COVID which led to the NIH RECOVER Initiative, the Office for Long COVID Research and Practice, the Long COVID Coordination Counsil, the Long COVID Federal Advisory Committe, the AHRQ Long COVID Care Network, amongst other federal efforts.
-
AHRQ Long COVID Care Network
-
NIH RECOVER Initiative Ancillary Studies
-
Coordination w/ the Office for Long COVID
-
Center for Medical Specialty Societies
-
Centers for Disease Control
-
Co-founded the Long COVID Alliance
-
Co-founded the Infection-Associated Chronic Conditions Initiative
-
Members of the Disability Economic Justice Collaborative
-
APHA Members and multi-year presenter and exhibitor
-
Drafted the Treat Long COVID Act, provided language to several other Long COVID and public health bills
-
and many more!
Nothing About Us, Without Us

With Patients
People living with Long COVID and disability know where the system fails—delayed diagnosis, poor care coordination, stigma, and inaccessible services. Their ideas surface the most urgent gaps early, ensuring priorities are grounded in reality, not theory. This builds trust and creates strategies that reflect actual needs, improving both patient outcomes and public health preparedness.
Plans shaped by patients are practical and sustainable. They anticipate fluctuating symptoms, fatigue, air-quality needs, transportation, and caregiving responsibilities. They focus on outcomes that matter—improved function, return to work or school, independence. This reduces program failure and strengthens health systems by lowering preventable ER visits and disability claims.
Recruitment designed by patients addresses stigma and distrust. It ensures compensation, accessibility, and outreach in diverse communities hardest hit by Long COVID and disability. This yields more representative data and equitable public health interventions.
Patients craft messaging that is credible, plain-language, culturally sensitive, and stigma-aware. It motivates people to recognize symptoms, seek care, and participate in research or programs. This reduces misinformation and improves public health by encouraging prevention and early intervention.
Patient facilitators bring empathy, cultural competence, and lived experience. They build safe spaces where participants feel heard and respected, fostering honest dialogue and stronger engagement. This results in higher-quality data and more effective solutions.
Patients provide context for interpreting data, ensuring measures reflect meaningful outcomes—fatigue reduction, cognitive improvements, daily functioning, return-to-work capacity. Their insights guide subgroup analyses that highlight disparities and prevent one-size-fits-all conclusions. This leads to actionable results for clinicians, policymakers, and communities.
Findings are translated into accessible resources for patients, caregivers, clinicians, schools, employers, and policymakers. Patients ensure knowledge is shared widely, leading to faster adoption of best practices, reduced stigma, and better care.
Patients hold stakeholders accountable, ensuring initiatives adapt, sustain momentum, and avoid being abandoned. This prevents resource waste, builds resilience, and creates durable public health infrastructure to respond to Long COVID and disability long term.
Without Patients
Brainstorming often results in misaligned goals or ableist assumptions. Resources are spent on projects with little community impact, leaving gaps unaddressed. The result: wasted funds, slower progress, and growing mistrust that undermines participation.
Programs collapse under real-world pressure. Patients drop out due to inaccessible timelines or criteria, and policy decisions rely on unrealistic measures. The outcome: wasted investments, inequitable access, and continued progression of illness and disability.
Recruitment skews toward healthier, wealthier participants, producing biased results. Communities most affected remain excluded, reinforcing inequities and leading to ineffective interventions.
Messaging risks being dismissive or inaccessible. It alienates communities, deters participation, spreads confusion, and allows misinformation to thrive—damaging both patient trust and population health.
Discussions risk becoming tokenistic or dominated by professionals unfamiliar with lived challenges. Participants disengage, key insights are missed, and outcomes lose credibility in the community.
Research defaults to surrogate markers that don’t translate into real-life improvements. Harm signals in vulnerable groups are overlooked. The result: interventions that look successful on paper but fail patients in practice.
Results stay siloed in journals or inaccessible reports. Communities, frontline providers, and the public remain uninformed, delaying uptake and fueling misinformation.
Programs stall, drift, or collapse when funding cycles end. Mistrust deepens, resources are squandered, and the cycle of inaction perpetuates worsening disability and higher costs.
The Consensus Long COVID Definition- N.A.S.E.M 2024 Adopted by HHS for Use Across the Whole of Government
Important Features of Long COVID
-
LC can impair individuals’ ability to work, attend school, take care of family, and care for themselves. It can have a profound emotional and physical impact on patients and their families and caregivers.
-
LC can range from mild to severe. It can resolve over a period of months or can persist for months or years.
-
LC can exacerbate pre-existing health conditions or present as new conditions.
-
LC can be diagnosed on clinical grounds. No biomarker currently available demonstrates conclusively the presence of LC
-
LC can follow asymptomatic, mild, or severe SARS-CoV-2 infection. Previous infections may have been recognized or unrecognized.
-
LC can be continuous from the time of acute SARS-CoV-2 infection or can be delayed in onset for weeks or months following what had appeared to be full recovery from acute infection.
-
LC can affect children and adults, regardless of health, disability, or socioeconomic status, age, sex, gender, sexual orientation, race, ethnicity, or geographic location.
Long COVID (LC) is an infection-associated chronic condition (IACC) that occurs after SARS-CoV-2 infection and is present for at least three months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems. LC can affect children and adults, regardless of health, disability, or socioeconomic status, age, gender, sexual orientation, race, ethnicity, or geographic location. LC can follow asymptomatic, mild, or severe SARS-CoV-2 infection and can be continuous from the time of acute SARS-CoV-2 infection or can be delayed in onset for weeks or months following what had appeared to be full recovery from acute infection.
LC can impact every organ system including the brain, gastrointestinal tract, heart, lungs, and immune system. It can last months to years to life, ranging from mild to severe and can present as singular or multiple symptoms and/or conditions such as, but not limited to, persistent fatigue, post-exertional malaise, difficulty concentrating, memory changes, recurring headache, dizziness, fast heart rate, sleep disturbance, migraine, stroke, blood clots, chronic kidney disease, postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis /chronic fatigue syndrome (ME/CFS), mast cell activation syndrome (MCAS), diabetes, and other autoimmune disorders such as lupus, rheumatoid arthritis, and Sjogren’s syndrome.

The Comprehensive Guide to Long COVID v2
Now in its second volume (first published in 2021), C19LAP’s Comprehensive Guide to Long COVID is the most complete, patient-developed resource for cross-sector stakeholders—patients and caregivers, clinicians, researchers, public-health officials, payers, employers, schools, and community leaders—built on five years of frontline, patient-led work. What sets this guide apart is its end-to-end usability (from bedside to policy), the credibility of lived experience paired with clinical rigor, and a cross-sector design that turns education into operations: documentation drives data, data informs policy, and policy allocates resources. Education is the hub of this entire cycle—without accurate, shared learning, care pathways stall, data quality erodes, and policy fails to meet need.















Take Action

Connect on TAPT: Exchange contact information & leave a google review
Request a Meeting with C19LAP
Express your Interest in joining a Long COVID Public Health Network
Help Recommend C19LAPs involvement in Long COVID Work
Support Our Mission
Your support is crucial. By partnering with us, donating, volunteering, or simply amplifying our message, you help us move the needle significantly. Each contribution empowers us to educate more clinicians and researchers, develop resources, enhance support services, and push for critical legislation and funding that can change lives. As we continue to grow and tackle the challenges of Long COVID, including mitigating future pandemics, your involvement enables us to maintain a robust dialogue with stakeholders and ensures that the Long COVID community's voice is heard and acted upon.

Via Check
COVID-19 Longhauler Advocacy Project, Inc.
P.O. Box 305
7491 N Federal Hwy C5
Boca Raton, FL, 33487